Sepsis is one of the most dangerous medical emergencies because it can move from vague early symptoms to organ failure in a matter of hours. Doctors know that fast treatment saves lives, but diagnosing sepsis is notoriously hard: fever, low blood pressure, and confusion can also appear in many other illnesses, and standard lab tests often take too long or do not give a clear answer. Researchers reporting in Nature describe a new microfluidic assay, a test that manipulates tiny amounts of liquid in chip-like channels, designed to spot sepsis from just a drop of blood. Instead of hunting directly for a single bacterium or inflammatory molecule, the test measures how a patient’s immune cells behave under stress. That matters because sepsis is not just an infection; it is the body’s overwhelming and damaging response to infection. By focusing on this immune response, the assay may capture a biological signature of sepsis that appears even when conventional cultures are still pending. If the approach holds up in larger studies, it could give clinicians a much faster way to decide who needs urgent antibiotics and intensive monitoring. The work points toward a future in which bedside blood tests do more than count cells or detect pathogens—they read the physical state of the immune system in real time.
Why sepsis is so hard to catch
Sepsis happens when the immune system’s attempt to fight an infection spirals into a body-wide inflammatory crisis. Blood vessels can become leaky, clotting can go wrong, and vital organs such as the kidneys, lungs, or brain can begin to fail.
The trouble is that early sepsis can look a lot like other conditions, from influenza to dehydration to a routine post-surgical reaction. Clinicians often rely on a combination of symptoms, blood chemistry, and microbiology cultures, but none of these alone gives a quick and definitive answer.
A blood test built on tiny channels
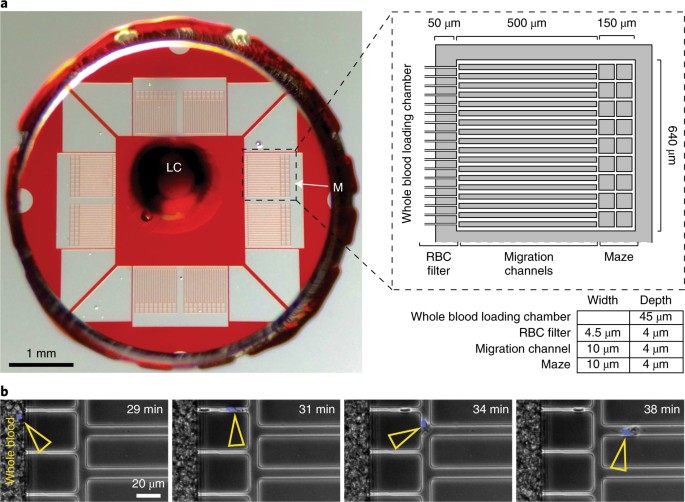
The new approach uses microfluidics, a technology that moves very small volumes of fluid through microscopic channels, often on a device the size of a credit card. Because it works with minute samples, it can potentially analyze blood quickly and with less preparation than conventional lab methods.
In this case, the researchers used the system to examine white blood cells, the immune cells that help detect and fight infection. Rather than simply counting those cells, the assay looks at measurable physical changes in them—how they deform, move, or respond as they pass through the device—which can reflect whether the immune system is in the abnormal state associated with sepsis.
Reading the immune system through cell mechanics
This idea may sound unusual, but cells are physical objects as well as biochemical ones. When white blood cells become activated during severe inflammation, their internal scaffolding, shape, and flexibility can change, and those changes may be detectable when the cells are forced through narrow channels or exposed to controlled stresses.
That makes the assay a kind of functional readout of immune status. Instead of asking only, “Is a pathogen present?” it asks, “Are this patient’s immune cells behaving like the cells of someone in sepsis?” That distinction is important because blood cultures can be negative even when a patient is critically ill, and because sepsis risk depends heavily on the host response, not just the microbe.
What the early results suggest
According to the report, the test was able to distinguish patients with sepsis from relevant comparison groups using a very small blood sample. The promise here is speed and practicality: a drop-of-blood assay could, in principle, fit into emergency departments, ambulances, or intensive care units where decisions need to be made fast.
Researchers are especially interested in tools that help sort ambiguous cases. A clinician facing a patient with fever and low blood pressure needs to know quickly whether the person is heading into sepsis, whether they need aggressive treatment now, and whether they should be watched more closely for deterioration.
What still needs to be proven
As encouraging as the concept is, early-stage diagnostic studies do not guarantee a test will work in routine care. Sepsis is a broad syndrome with many causes and severities, so any new assay must be validated in larger and more diverse patient populations, including older adults, children, and people with chronic illnesses that can alter immune cell behavior.
Researchers will also need to show how the test performs against current clinical workflows, not just in controlled research settings. A useful sepsis test must be reliable, easy to run, and able to improve real decisions—such as when to start treatment, when to escalate care, or when to avoid unnecessary antibiotics in patients who do not actually have sepsis.
Why This Matters
The biggest value of a faster sepsis test is time. Every hour of delay in recognizing and treating true sepsis can worsen outcomes, yet treating everyone “just in case” brings its own costs, including antibiotic overuse, side effects, and strain on hospital resources.
A tool that measures the body’s immune response from a tiny blood sample could help medicine move beyond blunt yes-or-no lab markers. It suggests a broader shift toward diagnostics that capture disease as a dynamic process, using the physical properties of cells as clues in the same way we now use genes, proteins, and imaging.
Where this could lead next
If future trials confirm the findings, microfluidic immune-cell assays could become part of a new generation of rapid bedside diagnostics for critical illness. The immediate goal would be better sepsis triage, but the larger opportunity is to build compact tests that read how the immune system is responding to trauma, infection, or inflammatory disease before irreversible damage sets in.
That is still a developing vision, not a finished clinical product. But the work described in Nature shows how a single drop of blood, combined with smart engineering, might eventually give doctors a much clearer picture of who is in danger and who needs help first.