A multicenter study from Poland offers a detailed look at how bullous pemphigoid, the most common autoimmune blistering skin disease, shows up in everyday clinical practice. Researchers reviewed 156 newly diagnosed patients seen between 2020 and 2024 across four dermatology departments and found a pattern that will be familiar to many doctors who treat older adults: most patients were elderly, most had several other health problems, and many arrived with intense itching before or alongside the more obvious skin damage. The study also examined whether some cases may be linked to recently started medications, a question that matters because drug-associated disease can be easy to miss in patients already taking many prescriptions. Nearly 15% of patients had begun a new drug within the six months before their symptoms started, suggesting that medication review should be part of the standard workup. At the same time, the researchers showed why lab testing remains central, especially direct immunofluorescence, a method that lights up disease-related antibodies in a skin sample much like a highlighter marks key text on a page. They paired that technique with enzyme-linked immunosorbent assay, or ELISA, and BIOCHIP-based indirect immunofluorescence to confirm diagnosis and compare clinical subgroups. Taken together, the findings paint a practical picture of who gets bullous pemphigoid, how they are treated, and where clinicians may need to look harder for triggers and faster diagnosis.
What the study set out to capture
Bullous pemphigoid, often shortened to BP, is an autoimmune disease in which the immune system mistakenly attacks structures that help anchor the outer layer of skin to the layers beneath it. When those connections weaken, the skin can separate and form tense blisters, erosions, and widespread itching.
The Polish team designed a retrospective cohort study, meaning they looked back at records from real patients rather than running a controlled trial. Their goal was simple but useful: describe the clinical profile of newly diagnosed BP, document how patients were treated, and identify cases that might be associated with recent drug exposure.
Who developed bullous pemphigoid
The 156 patients in the study were newly diagnosed between 2020 and 2024. Their mean age at diagnosis was 75.5 years, reinforcing the long-recognized fact that BP is mainly a disease of older adults.
Comorbidities were common. In fact, 78.85% of patients had at least one additional medical condition, with arterial hypertension, type 2 diabetes mellitus, and dyslipidemia appearing most often. That matters because these overlapping conditions can complicate both diagnosis and treatment, especially when symptoms might be confused with drug reactions, eczema, or infections.
How the disease appeared in real patients
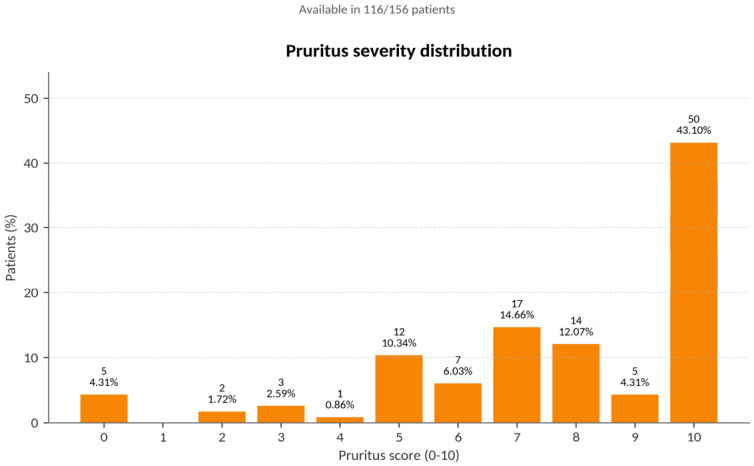
The most prominent symptoms were blisters and erosions, which are raw areas left after the skin surface breaks down. But one of the clearest takeaways is that severe itching was not a minor side issue; it was a major feature, reported in 74.14% of evaluated patients.
That detail is clinically important because BP does not always begin with dramatic blistering. Sometimes the disease starts more quietly, with persistent itch and inflamed skin, and only later progresses to the classic blistering picture. In everyday care, that can delay recognition, especially in older patients who already have several skin or systemic conditions.
Why diagnosis required more than a visual exam
Doctors did not rely on appearance alone. Diagnosis was based on clinical findings plus immunologic testing, including direct immunofluorescence, ELISA, and BIOCHIP-based indirect immunofluorescence.
Each test answers a slightly different question. Direct immunofluorescence looks at a skin biopsy to see whether antibodies are deposited in the tissue itself. ELISA measures antibodies in the blood against specific targets, such as BP180, a protein involved in skin adhesion. BIOCHIP-based indirect immunofluorescence uses prepared substrates to detect circulating antibodies in a more standardized panel format. Together, these methods help clinicians confirm that the immune system is attacking the skin in the characteristic way seen in BP.
The authors particularly emphasize the value of direct immunofluorescence in diagnostic evaluation. In practice, that makes sense: when symptoms are varied and patients are medically complex, a tissue-based test can provide a more solid anchor than clinical impression alone.
How patients were treated
The most frequently used therapy was topical glucocorticosteroids, medicines applied directly to the skin to calm inflammation and suppress the immune attack. These were followed by systemic glucocorticosteroids, which work throughout the body, and by methotrexate, an immunomodulating drug often used when steroid exposure needs to be reduced or the disease is harder to control.
This treatment pattern reflects a familiar tradeoff in BP care. Doctors need to control an uncomfortable and potentially serious disease, but they also need to be careful with medicines in older patients who may already have diabetes, high blood pressure, or other conditions that steroids can worsen.
The drug-associated subgroup
One of the study's most interesting questions was whether some cases were linked to medications started shortly before symptoms appeared. The researchers identified new drug exposure within six months before disease onset in 14.74% of patients.
These drug-associated cases were diagnosed in a shorter time than other cases. That could mean clinicians were more alert to the possibility of a medication trigger, or that the temporal link between starting a drug and developing symptoms made the pattern easier to spot.
The researchers also found that drug-associated cases showed lower positivity for BP180 on ELISA. However, that difference did not remain statistically significant after correction for multiple testing, which is a safeguard used when researchers compare many variables and want to reduce the chance of false-positive findings. In plain terms, the signal is interesting, but it is not strong enough here to treat as a firm biological difference.
Why This Matters
This study is useful because it describes BP as it appears outside the clean boundaries of a clinical trial. Real patients are older, often take many drugs, and rarely arrive with a textbook presentation. The finding that nearly 15% had recent new drug exposure does not prove causation in every case, but it does support a practical habit: review the medication list carefully whenever BP is suspected.
It also highlights how diagnosis should combine pattern recognition with laboratory confirmation. Severe itching, blistering, and erosions may point toward BP, but direct immunofluorescence and complementary antibody tests help separate it from look-alike conditions and may shorten the path to treatment.
What comes next
The study stops short of proving which drugs can trigger BP or how often those links are causal, but it gives clinicians a sharper map of the problem. Future work could sort patients by specific medication classes, track outcomes after stopping suspected drugs, and test whether earlier immunologic workups reduce delays in diagnosis. For now, the message is straightforward: in older adults with intense itch, blisters, or erosions, BP should stay high on the list, and both the biopsy slide and the prescription list deserve close attention.