Alpha-fetoprotein, usually shortened to AFP, is one of the most familiar blood markers used during pregnancy, but its role has grown far beyond its original use as a screening clue for fetal abnormalities. Produced mainly by the fetal liver and yolk sac, AFP passes into the amniotic fluid and then into the mother's bloodstream, where it can be measured with a simple blood test. For decades, clinicians have used abnormal AFP levels to help flag conditions such as open neural tube defects and certain chromosomal disorders. More recently, researchers have been looking at AFP in a broader way, asking whether it can also warn of problems rooted in the placenta, the temporary organ that nourishes the fetus during pregnancy. That shift matters because placental dysfunction is tied to major complications including preeclampsia, fetal growth restriction, preterm birth, and stillbirth. The picture that is emerging is more nuanced than a single high-or-low test result, with AFP acting as one piece of a larger risk puzzle rather than a stand-alone answer. In effect, AFP is evolving from a classic prenatal screening marker into a window on how well a pregnancy is functioning as a whole.
What AFP Measures in Pregnancy
AFP is a fetal protein, meaning it is made primarily by the developing fetus rather than the mother. During pregnancy, some of that protein crosses into maternal blood, which is why a maternal serum AFP test can provide indirect information about fetal and placental health.
In routine care, AFP is often interpreted relative to what is expected for a particular gestational age, since levels naturally change as pregnancy progresses. A result that is unexpectedly high or low does not diagnose a condition by itself, but it can tell clinicians that additional testing may be warranted.
Its Traditional Role in Prenatal Screening
The classic use of AFP has been in screening for open neural tube defects, serious birth defects in which the fetal brain or spinal cord does not close properly. When fetal tissues are more exposed, AFP can leak into amniotic fluid and maternal blood at higher-than-expected levels, making elevated AFP an important warning sign.
Low AFP, especially when considered alongside other blood markers, has also been linked to certain chromosomal abnormalities in the fetus. This is why AFP became part of multi-marker prenatal screening approaches, where it is interpreted together with ultrasound findings and other laboratory results rather than in isolation.
Beyond Genetics: A Marker of Placental Stress
The newer interest in AFP comes from studies suggesting that unexplained abnormal levels may reflect problems with the placenta. The placenta acts as the interface between mother and fetus, delivering oxygen and nutrients while removing waste, so even subtle dysfunction can have wide effects on pregnancy outcomes.
Researchers have reported associations between abnormal maternal AFP and obstetric complications such as preeclampsia, a dangerous condition involving high blood pressure and organ stress; fetal growth restriction, in which the fetus does not grow as expected; and preterm birth. The idea is not that AFP causes these problems, but that altered AFP may signal underlying damage, leakage, or abnormal development in placental tissues.
Why Interpretation Is Complicated
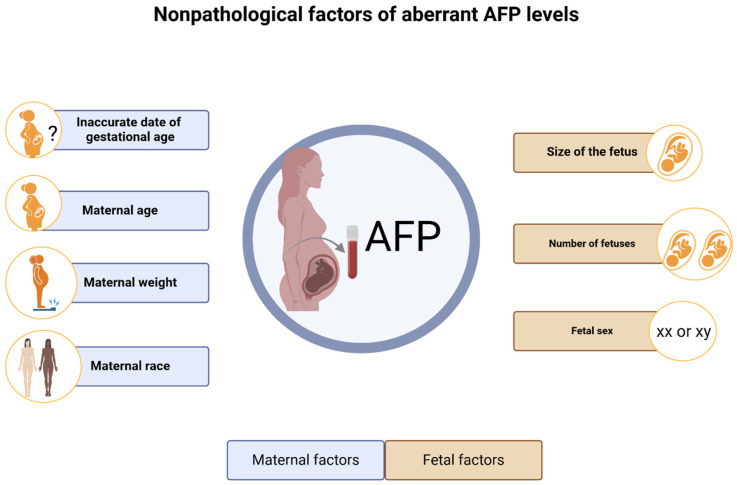
One reason AFP remains useful but imperfect is that many factors can influence the result. Incorrect dating of the pregnancy, multiple gestation, maternal weight, and certain fetal conditions can all shift AFP levels, which means clinicians must interpret the test in context.
That complexity is also why AFP has not become a universal stand-alone predictor of obstetric complications. A single biomarker rarely captures the full biology of pregnancy, particularly when different complications can arise from overlapping but distinct pathways involving blood flow, inflammation, and placental development.
How AFP Fits With Modern Prenatal Care
Today, prenatal care increasingly relies on combining information from blood tests, ultrasound, and clinical history to estimate risk. In that framework, AFP may be most valuable when it adds to a broader model that includes maternal characteristics, blood pressure, fetal growth measurements, and other placental markers.
This combined approach reflects a larger trend in obstetrics: moving from one-off screening toward layered risk assessment. Instead of asking whether AFP alone can predict a complication, researchers are asking whether it improves early detection when used alongside other data points that capture different aspects of pregnancy biology.
Why This Matters
The practical importance of AFP lies in timing. If clinicians can identify pregnancies at higher risk for complications earlier, they may be able to increase monitoring, adjust delivery planning, or intervene in ways that improve outcomes for both mother and baby.
That does not mean AFP is a crystal ball. Its value is as a relatively accessible, familiar biomarker that can help point clinicians toward pregnancies needing closer attention, especially in settings where more advanced testing may not be universally available.
What Comes Next
The most likely future for AFP is not a return to older screening models, but a more sophisticated role inside multi-marker prediction tools. As researchers refine how AFP interacts with other lab values and imaging findings, the test could help bridge the gap between traditional fetal anomaly screening and modern efforts to detect placental disease earlier.
For patients, that evolution means a long-used blood test may carry more information than once thought, though always with careful interpretation. For medicine, AFP remains a reminder that familiar biomarkers can gain new relevance when scientists look beyond their first application and ask what else they may be revealing about the biology of pregnancy.