Fast, dependable testing is one of the hardest problems in infectious disease control, especially when an outbreak is moving quickly or when testing has to happen outside a well-equipped lab. Standard methods such as qRT-PCR, the widely used molecular test that copies and detects genetic material, are accurate but often depend on expensive instruments, careful sample preparation, and trained technicians. That makes them harder to deploy in clinics with limited resources, at community testing sites, or in the field when speed matters most. A research team at the University of Toronto is working on a different approach: an automated microfluidic device that handles nearly the entire diagnostic workflow from sample to answer. The system combines microfluidics, which moves tiny amounts of liquid through miniature channels, with synthetic biology components that turn the presence of a pathogen into a glucose signal. That signal can then be read using a standard glucose meter, a cheap and familiar tool already used around the world. The goal is to make molecular diagnostics more portable, more automated, and easier to use without sacrificing the sensitivity needed to detect real infections. If that vision holds up in practice, it could help bring lab-grade pathogen testing much closer to the point of care.
How the platform works
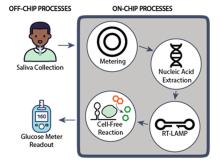
The Toronto team describes the device as a sample-to-answer system, meaning it is designed to take in a raw sample and produce a readable result without requiring the user to manage each step manually. Instead of moving tubes between different instruments, the test runs inside a single microfluidic platform that meters fluids, mixes reagents, and directs the sample through the workflow.
That matters because conventional molecular testing is often less limited by the chemistry than by the logistics around it. Even a strong assay can be difficult to use widely if it demands multiple preparation steps, separate machines, or a specialist to interpret the output.
From raw sample to amplified genetic signal
The system starts with sample metering, which means measuring out a controlled amount of the patient sample before processing. It then performs RNA extraction using a lysis buffer, a solution that breaks open cells or viral particles so their genetic material can be accessed.
After extraction, the device uses RT-LAMP, short for reverse transcription loop-mediated isothermal amplification. Unlike PCR, which requires repeated heating and cooling cycles, RT-LAMP amplifies RNA at a constant temperature, which makes it better suited for compact and lower-cost hardware. In this case, the reaction can be driven by a simple onboard heater rather than a full laboratory thermal cycler.
Synthetic biology as the readout
The most distinctive part of the platform is its detection system. Instead of relying on an optical reader or a bulky analyzer, the device uses a cell-free system, often abbreviated CFS, along with a toehold switch to convert the amplified pathogen signal into glucose.
A cell-free system is a biochemical toolkit made from the machinery of cells but used outside living cells, so it can carry out programmed reactions in a controlled test environment. A toehold switch is a synthetic RNA sensor designed to stay off until it encounters a matching genetic sequence; when the target is present, the switch activates the downstream signal. Here, that signal is glucogenic, meaning it produces glucose that can be measured directly.
Why glucose is a clever output
Using glucose as the final output solves a practical problem that has slowed many promising point-of-care ideas. Plenty of diagnostic concepts work in the lab, but they still require fluorescent scanners, cameras, or custom electronics to read the result, which makes real-world deployment harder and more expensive.
By translating the test result into glucose, the platform can use a standard glucose meter as the detector. That is a simple but powerful choice because glucose meters are inexpensive, widely available, easy to operate, and already familiar to health systems around the world. In effect, the team is repurposing an existing consumer medical device as the endpoint for molecular pathogen detection.
Why automation is the key engineering step
The promise of microfluidics is not just miniaturization. It is also automation: the ability to move tiny fluid volumes precisely, reduce contamination risk, and perform complex assay steps with very little user intervention. For a point-of-care test, that can be just as important as raw sensitivity.
Hands-free fluid manipulation could make the system more consistent across different users and settings. It also reduces the burden on clinics or temporary testing sites that may not have staff trained in molecular biology. In a pandemic or a fast-moving regional outbreak, that kind of simplicity can determine whether a test remains a niche tool or becomes something that can actually be deployed at scale.
Designed for outbreaks and emerging threats
The need for this kind of platform is not hypothetical. Recent years have shown how quickly testing bottlenecks can limit public-health response, and concerns about emerging threats such as H5N1 have kept attention focused on diagnostics that can move faster and closer to patients.
Point-of-care systems are especially valuable when centralized laboratory turnaround is too slow or geographically impractical. A compact platform that can extract RNA, amplify it, and report a result on-site could support hospitals, border screening, rural clinics, and outbreak investigations where speed and portability matter.
What still needs to be proven
As promising as the concept is, translational hurdles remain. Any point-of-care molecular test has to show not only that it works in controlled settings, but also that it is robust across real clinical samples, variable environmental conditions, and routine users who are not research specialists.
The platform will also need to demonstrate that its integrated workflow can maintain sensitivity and specificity, meaning it can correctly find true positives without generating too many false alarms. Manufacturing, cartridge stability, cost per test, and regulatory validation will all shape whether the system becomes a practical product rather than an elegant prototype.
Why This Matters
This work points to a larger shift in diagnostics: moving high-performance molecular testing out of specialized labs and into formats that are easier to use almost anywhere. By combining microfluidics, isothermal amplification, and synthetic biology with an everyday glucose meter, the University of Toronto team is tackling one of the biggest gaps in the field, which is not just detecting pathogens, but doing it in a way that is affordable and deployable.
If successful, systems like this could help public health respond faster, help clinicians make decisions sooner, and expand access to testing in lower-resource settings. The broader lesson is that innovation in diagnostics is often about integration as much as invention. The next generation of pathogen tests may win not because each individual component is brand new, but because the whole workflow is finally packaged into something simple enough to use where it is needed most.