A new microfluidic device, called the MPA-Chip, could make it easier to pull rare cancer cells out of a simple blood sample. The target is the circulating tumor cell, or CTC, a cancer cell that has broken away from a tumor and entered the bloodstream. These cells are medically important because their number and features can offer clues about whether a cancer is spreading, how aggressive it is, and whether treatment is working. In the reported study, researchers designed a chip filled with tiny pillar-like structures and tested several shapes to see which could best trap CTCs while letting most normal blood cells pass through. The winning design, a lozenge-shaped micropillar array, achieved more than 85 percent capture efficiency, more than 90 percent purity, and 97 percent cell viability, meaning most captured cells remained alive for further analysis. The team then used the device on blood samples from 12 breast cancer patients and found clear differences between non-metastatic and metastatic disease. They also observed that one metastatic patient showed a drop in captured CTCs during chemotherapy, suggesting the chip may be useful for tracking treatment response over time. Together, the results point to a compact, low-cost platform that could help turn blood-based cancer monitoring into something more practical for routine care.
A chip built to find extremely rare cells
CTCs are difficult to work with because they are vanishingly scarce. A standard blood sample contains billions of blood cells, but only a handful of tumor cells may be present, so any device meant to isolate them must be both selective and gentle.
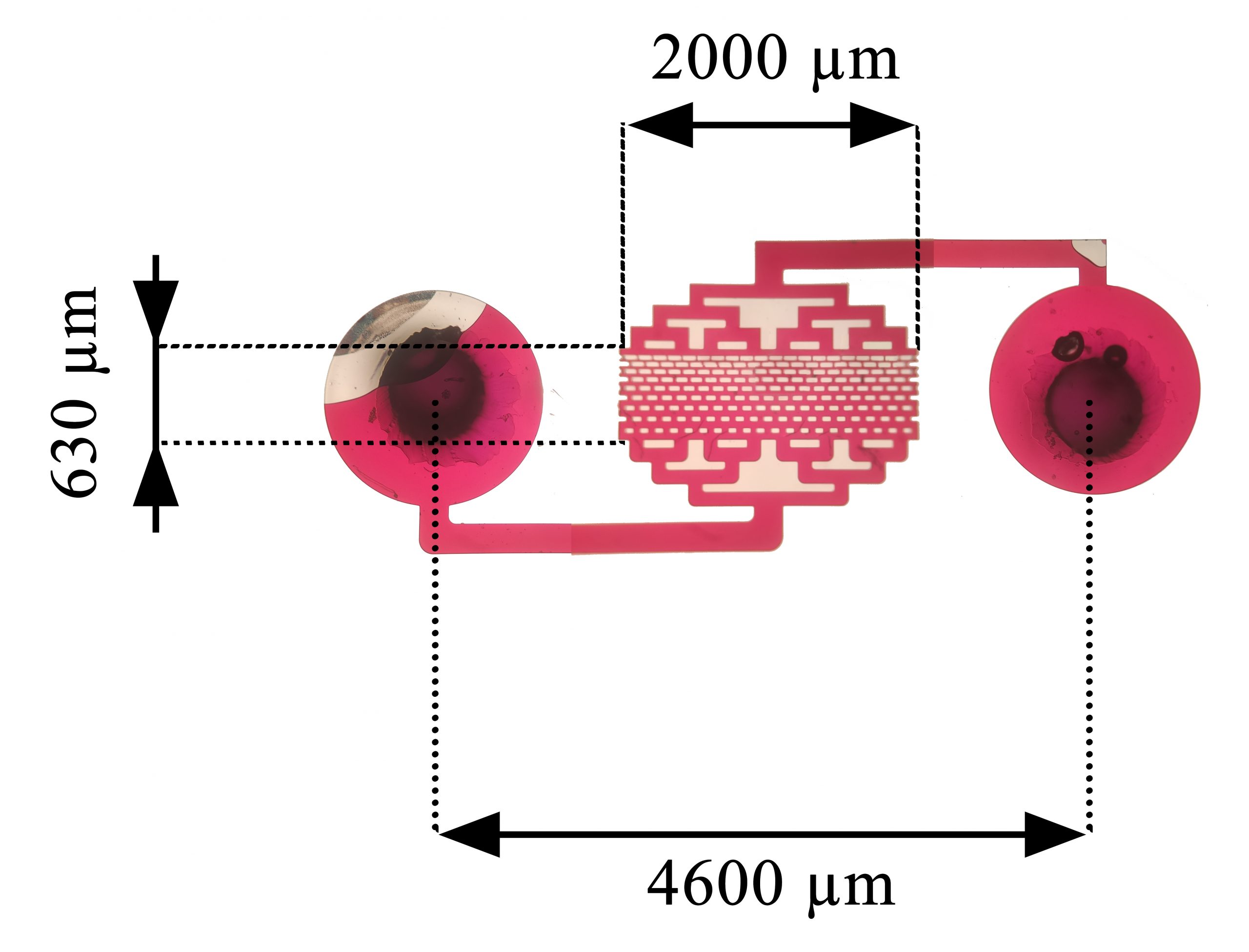
The new MPA-Chip approaches that problem through micropillar arrays, which are organized patterns of microscopic posts inside a fluid channel. As blood moves through the chip, the geometry of those pillars changes local flow conditions and increases the chance that larger or less deformable tumor cells will be captured.
Why pillar shape matters
The researchers did not settle on one design from the start. They fabricated chips with four different micropillar shapes: lozenge, rectangle, circle, and triangle, and compared how each one influenced fluid velocity, pressure, and cell capture.
That engineering step is important because tiny changes in geometry can strongly affect how cells behave in a microfluidic system. If the flow is too harsh, cells can be damaged; if it is too weak or poorly directed, the rare target cells may simply slip through.
Based on both simulations and experiments, the lozenge-shaped micropillars performed best. This design delivered a strong mix of efficiency, purity, and viability, suggesting it can trap CTCs effectively without excessively stressing them.
Testing with cancer cell lines and blood samples
Before moving to patient samples, the team evaluated the chip using breast and prostate cancer cell lines. Cell lines are laboratory-grown populations of cancer cells commonly used to test whether a new device behaves as expected under controlled conditions.
Those experiments helped establish that the chip could recover target cells reliably from complex samples. The reported performance, with capture efficiency above 85 percent and purity above 90 percent, is notable because recovery alone is not enough; a clinically useful sample also needs to be clean enough for imaging, staining, or downstream molecular analysis.
The chip also preserved 97 percent cell viability. That detail matters because living cells can potentially be cultured or studied further, opening the door to tests that go beyond simple counting and toward understanding how a patient's cancer might respond to specific therapies.
What the patient data showed
The most compelling part of the study came from validation in 12 patients with breast cancer. The chip detected CTCs in patients with both non-metastatic and metastatic disease, and the median counts differed markedly between the two groups.
Patients with non-metastatic disease had a median of 6 CTCs, while those with metastatic disease had a median of 25. That gap supports the idea that CTC burden can reflect disease state, with higher numbers associated with cancers that have spread beyond the original tumor site.
The study also described a metastatic patient whose CTC count dropped from 23 to 7 as chemotherapy continued. While that is only a single case, it hints at one of the biggest promises of liquid biopsy tools: the ability to track how treatment is working through repeated blood draws rather than relying only on imaging or invasive tissue biopsies.
A very small device with practical ambitions
One striking feature of the MPA-Chip is its size. The active area was reported as just 0.25 square centimeters, with a throughput of 0.5 milliliters per hour for a single chip.
That flow rate is modest, but the authors noted that throughput could be increased by running multiple chips in parallel. In practice, that kind of scalability matters because many promising lab-on-a-chip devices fail not because they do not work, but because they are hard to adapt to real clinical workflows.
The emphasis on a low-cost, practical, and efficient strategy also stands out. CTC technologies already exist, but many are expensive, technically demanding, or difficult to integrate into everyday use, so a simpler platform could lower barriers for hospitals and diagnostic labs.
Why This Matters
The broader significance of this work is that it pushes cancer monitoring toward a less invasive and more dynamic model. Instead of depending solely on tumor biopsies, which capture only one place and one moment in time, clinicians could potentially use blood to get repeated snapshots of how a cancer is changing.
That is especially relevant for metastatic disease, where tumors can evolve under treatment pressure. A tool that can isolate intact CTCs with high viability may allow not just counting, but also staining, characterization, and eventually culture, which could reveal which cells are most dangerous and how they differ from the primary tumor.
There is still a gap between a promising prototype and routine clinical use. The patient study here was small, and larger trials will be needed to show whether the chip can consistently predict prognosis, guide treatment decisions, or outperform existing methods.
Even so, the results are encouraging because they combine smart engineering with clinically meaningful signals. If future studies confirm these findings, compact micropillar chips like this one could become part of a new generation of blood-based cancer tools that help doctors monitor disease earlier, more often, and with less burden on patients.