Researchers report that the blood thinner enoxaparin, used at standard clinical doses, can make the oncolytic virus M1 infect bladder cancer cells more effectively and improve its antitumor activity in human bladder cancer models. Oncolytic viruses are viruses designed or selected to preferentially grow in cancer cells, where they can kill tumors directly and also stir up an immune response. In this study, the team found that enoxaparin did more than prevent clotting: it appeared to increase viral entry and spread in bladder cancer cells, leading to stronger cancer-killing effects when paired with M1. That matters because one of the biggest challenges for oncolytic virotherapy is getting enough virus into the tumor and keeping it active long enough to do meaningful damage. Bladder cancer is a logical target for this approach because the tumor is accessible and often treated locally, but many patients still need better options, especially when disease returns or stops responding to standard care. The work suggests that a familiar hospital drug could serve as a practical helper for viral therapy rather than requiring an entirely new platform. While the findings do not yet prove benefit in patients, they offer a specific, testable strategy for improving a promising cancer treatment with a medicine doctors already know how to use.
What the study found
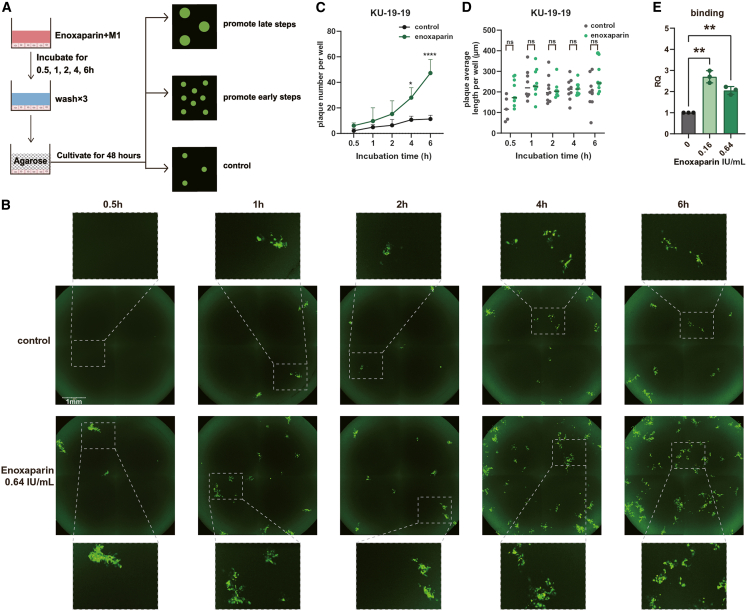
The central result is straightforward: adding enoxaparin boosted infection by the M1 virus in human bladder cancer. In turn, that stronger infection was linked to better antitumor effects, suggesting the anticoagulant was helping the virus do its job inside the tumor cells.
That is an unusual pairing on first glance. Enoxaparin is best known as a low-molecular-weight heparin, a class of drugs used to reduce dangerous blood clots, while M1 is being studied as an oncolytic agent. But cancer therapies often hinge on delivery, and a helper drug that improves access can be just as important as the main treatment itself.
Why viral infection is the bottleneck
You can think of an oncolytic virus like a key trying to get into a locked building. If only a few keys fit, or if they cannot reach enough doors, the therapy underperforms even if the virus is potent once inside. The study indicates enoxaparin may improve that first step by helping M1 gain more efficient access to bladder cancer cells.
For virotherapy, that early infection step shapes everything that follows. Better entry means more viral replication, more tumor-cell stress, and potentially more release of signals that alert the immune system to the cancer.
Why bladder cancer is a useful setting
Bladder cancer has long been a proving ground for local therapies. Doctors already treat some forms of the disease by delivering agents directly into the bladder, so it is a place where researchers can realistically imagine applying viral treatment in a targeted way.
Even so, better treatments are needed. Patients with aggressive or recurrent disease may exhaust standard options, and therapies that work through a different mechanism are especially valuable when tumors adapt to surgery, chemotherapy, or immune-based approaches.
What enoxaparin may be doing
The title points to a key mechanistic idea: a clinical dose of enoxaparin enhanced M1 infection, not just its downstream tumor-killing effect. In plain terms, the drug seems to be changing the conditions around the cancer cells in a way that lets the virus attach, enter, or spread more effectively.
That kind of effect is scientifically interesting because heparin-like molecules often interact with proteins on cell surfaces and in the surrounding matrix, the supportive material around cells. Like loosening a tightly woven net so a small object can pass through, enoxaparin may alter barriers that otherwise limit how well the virus reaches its target. The exact mechanism would need to be pinned down experimentally, but the study frames infection enhancement as the important first move.
Why using a familiar drug matters
Repurposing an established medicine can speed translational research, the phase where lab findings are pushed toward real-world care. Enoxaparin is already widely used in oncology and hospital medicine, so its dosing, side effects, and clinical handling are far better understood than those of a brand-new compound.
That does not make the combination automatically safe or effective in cancer patients receiving M1. It does, however, lower one practical barrier. Instead of inventing a new delivery enhancer from scratch, researchers may be able to build on a drug that clinicians already keep on the shelf.
What the results do and do not mean
The study supports the idea that combining enoxaparin with M1 could strengthen antitumor efficacy in bladder cancer, but preclinical success is not the same as patient benefit. Tumors in the body are more complex than cells in a dish, and combinations that look promising in controlled experiments can run into issues with dosing, safety, or inconsistent responses across patients.
There is also a balancing act unique to anticoagulants. If enoxaparin is used to help a viral therapy, investigators will need to make sure the potential gain in tumor control outweighs any added bleeding risk, especially in a cancer like bladder cancer where bleeding can already be part of the disease.
Why This Matters
This study highlights a simple but powerful idea in cancer therapy: sometimes the best way to improve a treatment is to help it get where it needs to go. Oncolytic viruses have attracted attention for years because they can attack tumors in a highly selective way, yet delivery and infection efficiency remain stubborn obstacles. If enoxaparin truly improves M1 infection at doses already used in clinics, that could make viral therapy more practical and more potent without changing the virus itself.
The broader significance goes beyond bladder cancer. Many advanced therapies, from viruses to nanoparticles, fail not because the core concept is weak but because they cannot navigate the body well enough to reach their target. Studies like this one push the field to think harder about companion drugs that tune the tumor environment and give promising therapies a better chance to work.
What comes next
The next step is careful validation in more advanced models and, if the evidence holds up, clinical testing that measures both efficacy and safety. Researchers will want to identify which patients are most likely to benefit, how timing and dose affect viral infection, and whether the combination can work alongside other bladder cancer treatments. If those questions can be answered, a common anticoagulant could become an unexpectedly useful tool for boosting oncolytic virotherapy.