A rare autoimmune disorder linked to anti-SEZ6L2 antibodies appears to cause far more than clumsy movement or balance problems. In a new case report paired with a systematic review, researchers describe a 45-year-old man with a severe, fast-developing cerebellar syndrome and show that his cerebellum kept shrinking over time on brain scans despite immunotherapy. The work also pulls together every published case the authors could find, offering one of the clearest pictures yet of what this syndrome looks like in real patients. Across 22 total cases, all patients had cerebellar symptoms, but many also developed parkinsonism, cognitive changes, and psychiatric symptoms, suggesting a broader brain disorder than clinicians may expect at first glance. The review found that most patients were left with substantial disability even when some symptoms improved. That matters because the condition is rare enough to be missed, especially early on, when it may resemble other forms of ataxia, a term for poor coordination caused by damage to the brain's movement centers. The study's most striking detail is the imaging evidence: the cerebellum, which helps fine-tune movement and supports aspects of thinking and emotion, showed progressive atrophy while the rest of the brain stayed largely within normal range. Taken together, the report suggests anti-SEZ6L2 syndrome is a severe immune-mediated neurologic disease that deserves earlier recognition and more careful long-term monitoring.
A rare antibody with a distinct pattern
SEZ6L2 stands for seizure-related 6 homolog like 2, a protein associated with nerve cells. When the immune system makes antibodies against it, the result can be an immune-mediated cerebellar syndrome, meaning the body's own defenses appear to interfere with the cerebellum and related brain functions.
If the cerebellum is the brain's quality-control system for motion, anti-SEZ6L2 syndrome seems to jam that control panel. Patients do not just become unsteady; they can also develop slowed movements, stiffness, changes in thinking, and shifts in mood or behavior.
The new case: severe symptoms and lasting disability
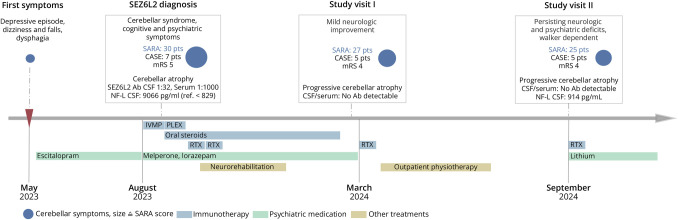
The featured patient was a 45-year-old man who developed a severe subacute cerebellar syndrome, meaning his symptoms worsened over weeks to months rather than appearing in a single stroke-like moment or over many years. Along with major coordination problems, he had cognitive, psychiatric, pyramidal, and parkinsonian features, pointing to involvement beyond the cerebellum alone.
The severity was high by standard neurologic measures. His peak SARA score, a scale used to quantify ataxia, reached 30, and his peak modified Rankin Scale score, which measures overall disability, reached 5, indicating profound functional impairment.
What brain volumetry revealed
The researchers also performed serial MRI volumetry, which is a way of measuring the size of brain structures over time rather than simply looking at scans by eye. Think of it like checking not just whether a plant looks smaller, but using a ruler repeatedly to document exactly how much it has shrunk.
That approach showed progressive cerebellar atrophy, or tissue loss, relative to age-matched and sex-matched healthy controls. At the same time, whole-brain and subcortical volumes stayed within the normal range, suggesting a particularly selective pattern of damage centered on the cerebellum.
What the literature review found
To place the case in context, the authors conducted a PRISMA-compliant systematic review of MEDLINE and EMBASE and identified 21 previously published patients. Including the new case, that brought the total to 22 patients with anti-SEZ6L2 syndrome.
Every patient had a cerebellar syndrome, confirming that this is the core feature of the disease. But the review also showed that so-called noncerebellar symptoms were common: cognitive symptoms appeared in 14 of 22 patients, or 64%; parkinsonism in 8 of 22, or 36%; and psychiatric symptoms in 6 of 22, or 27%.
Imaging, spinal fluid, and tumor links
Brain imaging added another consistent clue. Cerebellar atrophy was reported in 19 of 22 patients, or 86%, which fits with the new case's longitudinal MRI findings and suggests that visible cerebellar tissue loss is not an exception but a recurring feature.
Other tests were less uniformly abnormal. Cerebrospinal fluid, the clear liquid surrounding the brain and spinal cord, showed pleocytosis, an increase in immune cells that signals inflammation, in 7 of 21 patients, or 33%. Two patients had tumors that were temporally associated with the syndrome, raising the possibility that in some cases the immune response may be linked to cancer.
Treatment helps some, but often not enough
The patient in the case report received sequential immunotherapy, but the gains were limited. He improved only mildly, and substantial disability remained, even as treatment presumably aimed to calm the immune attack.
The broader review paints a similar picture. Among seven patients with SARA data, the median peak score was 27 and improved to 20 at follow-up, which suggests some reduction in ataxia severity. But among 11 patients with modified Rankin Scale data, the median score remained 4 both at peak disease and follow-up, indicating that many people were still significantly disabled in daily life.
Why This Matters
Rare neurologic autoimmune diseases are often diagnosed late because they mimic more familiar disorders. This study suggests anti-SEZ6L2 syndrome should be considered when a patient develops rapidly progressive ataxia, especially if it comes with parkinsonism, cognitive decline, or psychiatric symptoms rather than a pure movement problem.
The paper also shows why better measurement matters. Standard exams can tell doctors whether a patient walks better or worse, but longitudinal volumetry can reveal ongoing structural damage in the cerebellum even when the rest of the brain looks preserved, potentially helping clinicians track disease progression more precisely.
A clearer picture, but many open questions
Because the syndrome is so rare, the evidence base still comes from case reports and small series, which limits what anyone can say about the best treatment or the most reliable predictors of recovery. Even so, this synthesis sharpens the clinical picture: anti-SEZ6L2 syndrome is typically severe, often broader than a simple cerebellar disorder, and may leave lasting disability despite partial improvement.
The next step is straightforward in concept but hard in practice: find more patients earlier, collect standardized imaging and outcome data, and learn which therapies can actually halt the cerebellum's decline rather than only soften symptoms. For now, the study gives neurologists a more concrete map of a rare disease that can otherwise hide in plain sight.