CAR-T cells have transformed treatment for some blood cancers, but they have struggled to deliver the same results in solid tumors. This article argues that one major reason is not just biology in the classic sense, but physics: the cells often cannot move effectively through the dense, cramped architecture of tumor tissue. The authors focus on microfluidics, a technology that uses tiny channels to mimic the microscopic environment inside the body, as a way to study this problem in far more realistic detail than standard lab assays allow. In solid tumors, therapeutic T cells must leave blood vessels, squeeze through narrow spaces, navigate stiff extracellular material, and remain functional while under mechanical stress. Those steps are easy to overlook when migration is tested in flat dishes or simple gels. By highlighting physical confinement as a central barrier, the paper reframes poor CAR-T performance as a problem of access as much as recognition. It also suggests that better models could help researchers design therapies that are not only potent killers, but better travelers. For biochip and microfluidics researchers, that makes this review a useful map of where engineering can directly shape the future of immunotherapy.
Why solid tumors are so hard for CAR-T cells
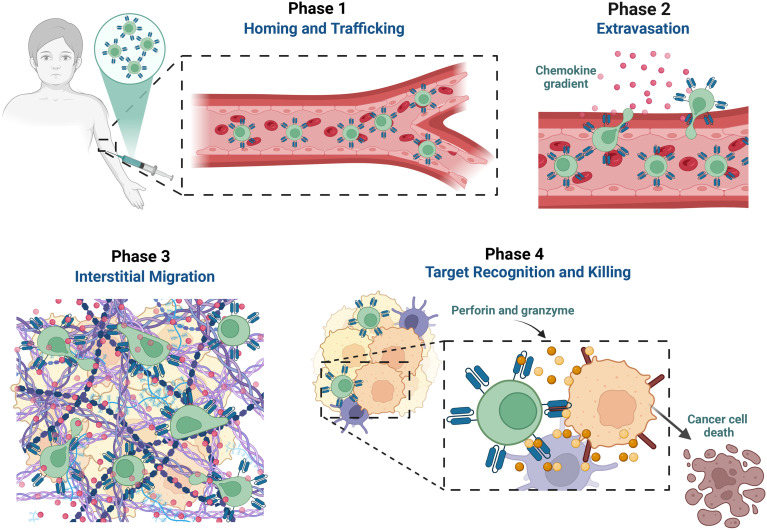
CAR-T therapy works by taking a patient's T cells, engineering them to express a chimeric antigen receptor, and returning them to the body so they can seek out cancer cells. In leukemia and lymphoma, these targets are often relatively accessible because the malignant cells circulate in blood or reside in more open immune environments.
Solid tumors are different. They are packed with cancer cells, supporting stromal cells, tangled proteins known as the extracellular matrix, abnormal blood vessels, and chemical signals that suppress immune function. Even if a CAR-T cell can recognize its target, it may still fail because it cannot efficiently reach enough tumor cells deep inside the mass.
The overlooked role of physical confinement
The review's central message is that physical confinement deserves far more attention. This term refers to the tight spaces, pores, channels, and mechanical obstacles that immune cells encounter as they move through tissue. In many solid tumors, those spaces are simply smaller, stiffer, and more irregular than what T cells are built to navigate comfortably.
That matters because migration is not passive drifting. T cells constantly deform their membranes, reorganize their internal skeleton, and generate pushing and pulling forces to move forward. When the surrounding architecture is too restrictive, movement slows, exhaustion can increase, and the cells may lose time and energy before they ever engage the tumor.
Why standard lab models fall short
Traditional migration studies often rely on two-dimensional surfaces, porous inserts, or bulk gels. These tools are useful, but they usually simplify the mechanical landscape so much that key barriers disappear. A cell that looks highly mobile in a standard assay may behave very differently when forced to squeeze through channels that resemble real tumor spaces.
That gap helps explain why promising preclinical findings do not always translate into clinical success. If a model does not capture confinement, stiffness gradients, vessel-like entry points, or the geometry of matrix fibers, it may overestimate how well engineered T cells can infiltrate a tumor.
What microfluidic systems add
Microfluidic devices are especially powerful because they let researchers build miniature environments with precise control over size, shape, flow, and mechanical resistance. A chip can include channels narrow enough to test squeezing behavior, compartments that mimic blood vessels and tumor regions, or gradients of signaling molecules that guide immune-cell movement.
That level of control allows scientists to separate variables that are usually tangled together in living tissue. Researchers can ask whether a CAR-T cell is failing because of weak chemotaxis, meaning movement toward a chemical cue, because of poor deformation in tight spaces, or because repeated confinement changes its activation state. Those are hard questions to answer cleanly in animal models alone.
Linking mechanics to cell function
One of the most interesting ideas in the review is that migration and killing should not be treated as separate abilities. A T cell that spends too long struggling through constricted spaces may arrive at its target in a weakened state. Mechanical stress could alter signaling, metabolism, or persistence, all of which influence therapeutic performance.
This means future CAR-T optimization may need to go beyond target choice and receptor design. Researchers may also need to engineer cells for improved motility, deformability, resistance to suppressive mechanics, or better coordination with matrix-remodeling strategies that open physical paths into tumors.
Implications for device design and therapy development
For bioengineers, the review points toward more sophisticated chip models that combine confinement with other real tumor features. The most informative platforms may integrate stromal cells, extracellular matrix composition, fluid flow, oxygen gradients, and tumor-derived signals rather than testing each in isolation. That would create a more faithful picture of what CAR-T cells actually face in patients.
These platforms could also become practical screening tools. Instead of evaluating candidate cell products mainly by how strongly they kill targets in easy conditions, developers could rank them by how well they infiltrate, survive mechanical stress, and sustain function in tumor-like microenvironments. That would make preclinical testing more predictive and potentially reduce costly dead ends.
Why This Matters
The review matters because it shifts the conversation from a purely biochemical view of immunotherapy to a biophysical one. In solid tumors, success depends not only on whether a CAR-T cell knows what to attack, but whether it can physically get there. That is a simple idea, yet it has major consequences for how therapies are designed, tested, and compared.
It also highlights why microfluidics belongs at the center of cancer immunotherapy research. Biochips can expose hidden failure points long before a therapy reaches the clinic, helping scientists redesign cells or combinations with more realistic goals. If physical confinement is a key bottleneck, then devices that measure and manipulate that bottleneck become essential translational tools, not niche lab gadgets.
What comes next
The field now has an opportunity to build a new generation of tumor-on-chip systems tailored specifically to immune-cell trafficking. The most valuable models will likely connect mechanics with live readouts of signaling, exhaustion, cytotoxicity, and long-term persistence. If that happens, microfluidics could help turn CAR-T therapy for solid tumors from an immunology challenge into an engineering problem that can be systematically solved. The broader lesson is compelling: in cancer therapy, getting to the target can be just as important as recognizing it once you arrive.