A growing body of research suggests that neuroinflammation—the brain’s immune response—may play a meaningful role in at least some cases of autism spectrum disorder, or ASD. Rather than treating autism as a single condition with one cause, scientists increasingly describe it as a collection of related neurodevelopmental differences shaped by genetics, environment, and biology that can vary widely from person to person. This review examines one of the most actively studied biological threads: how immune signaling, inflammatory molecules, and altered activity in brain support cells might influence brain development and behavior. It also looks at the drug strategies now being explored to calm or redirect those pathways, from broad anti-inflammatory compounds to more targeted approaches aimed at specific immune signals. The central idea is not that inflammation explains all of autism, but that it may define a biologically important subgroup of patients who could benefit from more personalized treatment. That matters because current therapies mainly address behavior and daily functioning, while no approved medicines directly target autism’s core biology. By connecting inflammatory mechanisms to emerging pharmacology, the article maps out where the science is becoming more precise—and where major uncertainties still remain.
How Inflammation Enters the Autism Picture
ASD is usually diagnosed based on social communication differences and repetitive or restricted behaviors, but those outward features can arise from many different biological routes. Researchers have increasingly focused on the immune system because studies have found abnormal levels of inflammatory molecules in some people with autism, along with signs of altered immune activity in blood, cerebrospinal fluid, and brain tissue.
One recurring theme is the role of cytokines, which are signaling proteins the immune system uses to coordinate responses. Several studies have reported changes in cytokines such as interleukins, tumor necrosis factor, and other inflammatory mediators in autistic individuals, raising the possibility that persistent low-grade inflammation could affect how neural circuits form and function.
The Brain’s Immune Cells May Be Involved
A key player in this story is the microglia, the brain’s resident immune cells. Microglia normally help sculpt the developing brain by clearing debris, responding to injury, and pruning unused synapses—the connections between neurons. If those cells become overactive or behave abnormally during development, they could influence connectivity in ways that affect behavior, learning, and sensory processing.
Astrocytes, another type of support cell in the brain, may also contribute. These cells help regulate neurotransmitters, maintain the blood-brain barrier, and support metabolic balance, so inflammatory changes in astrocytes could ripple across many aspects of brain function. Together, microglia and astrocytes form a plausible bridge between immune disturbance and altered neurodevelopment.
Inflammatory Pathways Are Complex, Not One-Dimensional
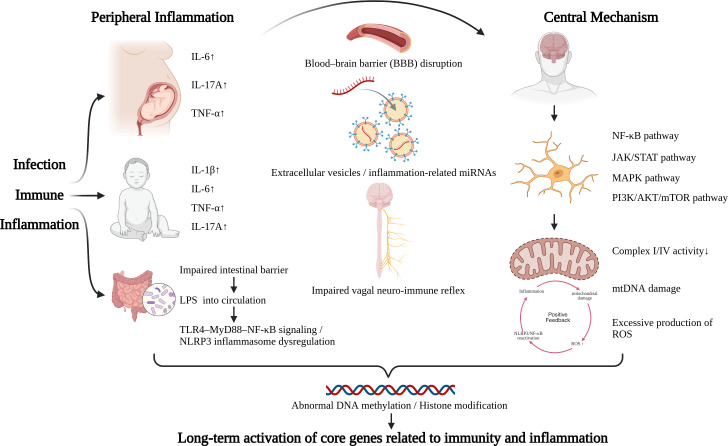
The review emphasizes that neuroinflammation in ASD is unlikely to be a simple on-off switch. Instead, it appears to involve overlapping pathways tied to oxidative stress, mitochondrial dysfunction, disrupted gut-immune signaling, and changes in the permeability of the blood-brain barrier, the protective interface that helps control what enters brain tissue from the bloodstream.
That complexity helps explain why findings in the field can seem inconsistent. Not every person with autism shows the same inflammatory profile, and some studies may be capturing different subtypes, different ages, or different stages of development. In practice, this means inflammation is best understood as one biological dimension within ASD rather than a universal explanation.
What Drug Developers Are Trying
Because standard autism care focuses largely on behavioral therapies and treatment of associated symptoms, researchers are exploring whether anti-inflammatory or immune-modulating drugs could help selected patients. Some candidates are familiar medications repurposed from other fields, while others are more experimental compounds designed to act on specific molecular targets.
Broad approaches include agents with antioxidant and anti-inflammatory properties, which aim to reduce damaging immune activation without requiring an exact diagnosis of the pathway involved. More targeted approaches try to block particular cytokines, regulate microglial activation, or influence signaling networks linked to inflammation and synaptic function. The appeal is precision: if a measurable immune abnormality is present, treatment could in theory be matched to that biology.
The Promise and Limits of Targeted Interventions
The review describes progress in pharmacological strategies, but it also makes clear that the field is still early. Some small studies and preclinical models have suggested benefits from compounds that dampen inflammatory signaling, improve mitochondrial performance, or reduce oxidative stress, yet results are not uniform and often come from limited patient groups.
This is a crucial point for families and clinicians. A treatment that helps one inflammatory subtype of ASD may do little for another person whose symptoms are driven mainly by different mechanisms. That is why the future likely depends less on finding one “autism drug” and more on identifying biomarkers—measurable biological signals—that can show who is most likely to respond.
Why Biomarkers Matter So Much
Biomarkers could include cytokine patterns in blood, imaging signs of glial activation, metabolic signatures, or other indicators of immune dysregulation. Without those tools, clinical trials risk mixing together very different patient populations, which can make a potentially useful treatment look ineffective overall.
The move toward biomarker-guided treatment mirrors what has happened in cancer and some autoimmune diseases, where therapy increasingly depends on matching drugs to underlying biology. For autism, that shift would be especially important because the diagnosis is behavior-based, while the biology beneath it is highly heterogeneous.
Why This Matters
This review matters because it pushes the autism field toward a more mechanistic and personalized framework. Instead of debating whether inflammation causes autism in a broad, all-or-nothing way, it asks a more useful question: when and in whom do inflammatory pathways contribute enough to become a therapeutic target?
That reframing could improve both science and care. It encourages researchers to define biologically meaningful subgroups, design smarter clinical trials, and avoid overpromising treatments based on early or incomplete evidence. It also offers a path toward interventions that address underlying physiology rather than only managing downstream symptoms.
What Comes Next
The most likely next step is not a single breakthrough drug but a gradual tightening of the link between immune biology and treatment selection. Future studies will need larger cohorts, standardized biomarker panels, and longer follow-up to determine whether immune-targeted therapies produce durable improvements in communication, behavior, or quality of life.
If that work succeeds, neuroinflammation could become one of the first clear examples of precision medicine in autism: not a universal answer, but a targeted strategy for the people whose biology points in that direction. For now, the field’s real advance is conceptual—moving from broad speculation about inflammation to a more testable roadmap for intervention.