Point-of-care diagnostics are tests designed to deliver answers where the patient is, rather than sending samples away to a central lab. The article argues that this field is being reshaped not just by better chemistry and smaller instruments, but by the arrival of consumer electronics, wireless connectivity, and data analytics. That mix matters because it could make testing faster, more widely available, and more tightly linked to treatment decisions, especially outside traditional hospitals. Instead of thinking about diagnostics as isolated gadgets, the piece frames them as part of a connected ecosystem that can move information between patients, clinicians, and health systems in real time. It also suggests that healthcare may shift as these tools improve, with diagnosis and care decisions happening in decentralized settings such as clinics, homes, and remote sites. At the same time, the article is careful to note that the road to broad adoption will depend on combining this new digital energy with long-standing scientific work in analytical chemistry, the science of detecting and measuring substances, and microfluidics, the control of tiny volumes of liquid in small devices. The result is a picture of a field in transition: technically promising, commercially energized, and likely to change how medicine is delivered if its practical constraints are handled well.
A field boosted by digital tools
The core claim of the article is simple: point-of-care, or POC, diagnostics have entered a new phase because they can now borrow power from technologies built outside medicine. Smartphones, low-cost sensors, cloud software, and always-on internet connections have given developers new ways to design and deploy tests.
A useful analogy is the shift from a standalone camera to a smartphone camera. The lens still matters, but what makes the device far more useful is the surrounding system: storage, connectivity, computing, and apps. In the same way, a modern POC diagnostic is no longer just a chemical assay in a plastic cartridge; it can also be a data-producing node in a broader healthcare network.
Why the old science still matters
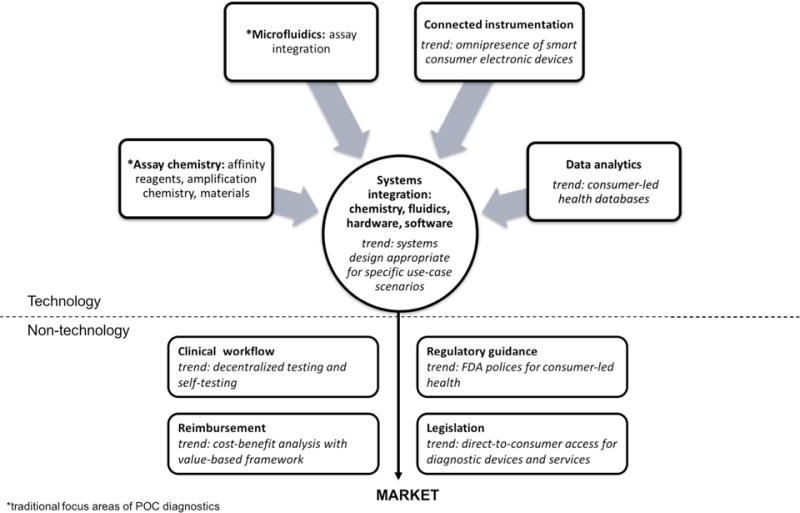
The article does not treat software as a substitute for the underlying test. It emphasizes that the future of POC diagnostics will depend on a marriage between digital capabilities and the traditional scientific disciplines that make a measurement trustworthy in the first place.
That means the quality of the chemistry and fluid handling still sets the floor for performance. If a test cannot reliably detect a biomarker, meaning a measurable sign of disease, no amount of connectivity can fix that. The digital layer adds speed, access, and coordination, but the measurement itself still has to be sound.
From central labs to decentralized care
One of the article's biggest themes is decentralization. Rather than requiring patients to travel to a hospital or wait for samples to move through centralized laboratories, connected POC devices could support diagnosis and treatment selection in many different settings.
That includes physician offices, community clinics, remote sites, and even the home. For clinicians, the appeal is practical: faster results can compress the time between suspicion of disease and a treatment decision. In areas where specialist care or laboratory infrastructure is limited, that speed can also reduce the friction that keeps patients from getting timely care.
A different healthcare value chain
The piece also points to a larger economic and clinical shift. As therapies become more personalized, increasingly tied to an individual's genetics or biomarkers, diagnostics may take on a more central role in deciding what treatment should happen and when.
Seen this way, diagnostics become more than a preliminary step before therapy. They become a gatekeeper for precision medicine, helping determine which drug fits which patient and whether a treatment is working. The article suggests this could move more value toward accurate, accessible testing rather than placing most of the system's emphasis on the treatment alone.
Connection creates opportunity, and new risk
Connectivity is presented as a source of momentum, but also of complexity. When a POC device can send data to clinicians, electronic records, or decision-support software, the test becomes part of a larger information flow that can improve follow-up and care coordination.
But connected devices also raise questions about reliability, integration, and data handling. A lab machine tucked inside a hospital has one kind of operating environment; a test used in a home, a nonprofit clinic, or a field setting has another. The more these tools spread across settings, the more their designers have to account for real-world variability, not just ideal lab conditions.
Not all point-of-care settings are the same
A particularly sharp insight in the source is that common labels such as home, clinic, field, and hospital do not capture the full reality of POC use. The authors argue that infrastructure and budget should be separated rather than treated as if they always travel together.
That distinction matters because two sites may both be called clinics while facing very different constraints. A nonprofit clinic in a low- and middle-income country may be geographically remote and cost-sensitive, while a clinic in a military context may be just as remote from central lab facilities but operate with very different budget assumptions. Lumping them together can lead developers to design for the wrong use case.
Designing for context, not just category
The same logic applies beyond clinics. A device intended for global health field use may share some logistical challenges with a monitoring device used far from a hospital in another setting, but the needs are not identical. Power supply, staffing, supply chains, training, maintenance, and acceptable test cost can all differ.
This is where the article pushes the conversation beyond simple enthusiasm. A successful point-of-care test is not just analytically strong; it has to fit its environment. In practice, that means developers and healthcare systems must define the setting carefully before deciding what a device should measure, how much it can cost, and what kind of connectivity it needs.
Why This Matters
The article's larger significance is that it treats point-of-care diagnostics as infrastructure for a new style of medicine. If testing becomes portable, connected, and accurate enough for everyday clinical decisions, care can move closer to the patient while still staying linked to professional oversight and digital records.
That has implications for infectious disease, chronic disease monitoring, and personalized treatment selection. It also matters for equity: a test that works well in a central hospital but fails in low-resource or remote settings does little to expand access. By insisting on both technical rigor and careful attention to context, the article sketches a more realistic path toward wider adoption.
Looking ahead, the most durable advances in point-of-care diagnostics will likely come from teams that blend chemistry, engineering, software, and healthcare delivery expertise. The connected age gives the field new tools and new investment, but adoption will depend on whether devices can produce reliable answers in the messy places where people actually receive care. If that balance is achieved, diagnostics may become one of the main ways medicine grows faster, more personalized, and less tied to the walls of the central lab.