Point-of-care testing, or diagnostics performed close to the patient, is moving from a convenience to a core public-health tool. In the reviewed article, the authors argue that faster, more portable tests could change how outbreaks are detected, tracked, and contained by shifting diagnosis away from distant central laboratories and toward clinics, field sites, farms, and food systems. That matters because infectious-disease control often depends on speed: the sooner a pathogen is identified, the sooner treatment, isolation, tracing, or environmental cleanup can begin. The piece also broadens the discussion beyond the bedside to point-of-need testing, a term used for on-site testing of animals, food, and environmental samples where disease threats may first appear. Instead of waiting for samples to travel to high-throughput reference labs with expensive equipment, health workers could use compact tools that deliver answers where decisions are being made. The review highlights two main technical paths: tests that read a pathogen's genetic material and tests that detect its immune signature, such as antigens or antibodies. It also points to a newer frontier, metagenomic diagnostics, which look broadly at all genetic material in a sample rather than searching for one suspected target. Taken together, the article makes a simple case with big implications: portable diagnostics could strengthen surveillance, especially in low-resource settings where electricity, specialized staff, and advanced instruments are limited.
Why centralized testing is often too slow
Traditional infectious-disease diagnostics usually depend on centralized laboratories. These facilities are powerful and can process many samples, but they also require complex instruments, trained specialists, and reliable infrastructure.
That setup works well when time is not critical, but outbreaks rarely offer that luxury. Shipping samples, waiting in queues, and returning results to frontline workers can slow action at the exact moment when quick decisions matter most.
What point-of-care and point-of-need really mean
The review draws an important distinction between two closely related ideas. Point-of-care testing, or POCT, generally refers to testing human patients near where care is delivered, such as at the bedside, in a clinic, or in a community setting.
Point-of-need testing, or PONT, casts a wider net. It includes on-site testing outside traditional clinical care, such as in animals, food supplies, or environmental samples, although the authors note that the term is still not fully standardized.
How these tests work in practice
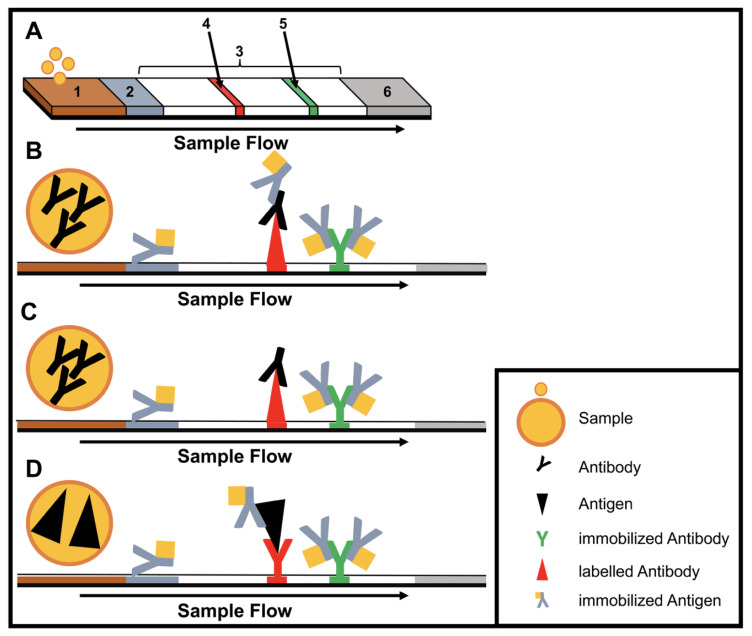
Most portable diagnostic tools follow one of two basic strategies. Some use immunological methods, which detect antigens from a pathogen or antibodies produced by the host immune system; think of these as molecular name tags that reveal whether the body has seen a particular invader.
Others identify the pathogen at the genomic level by reading pieces of its DNA or RNA, the genetic instructions that make each microbe distinct. That is more like matching fingerprints than spotting a badge, and it can offer more direct evidence of which organism is present.
The rise of field-ready molecular testing
The authors describe a shift now underway: while immunoassays still dominate many rapid tests, portable molecular methods are gaining ground. This is a meaningful change because genetic detection can improve specificity, helping users distinguish one pathogen from another even when symptoms look similar.
The review also flags the emergence of field protocols for metagenomics. In simple terms, metagenomics does not ask only, "Is pathogen X here?" It asks, "What genetic material is in this sample?" That broader view can be especially useful when the cause of an outbreak is uncertain.
Where portable diagnostics already show their value
The article points to malaria and human immunodeficiency virus, or HIV, as clear examples of rapid diagnostics used in the field. In these settings, faster testing has already helped improve disease control and has supported changes in treatment and patient care.
That benefit is particularly strong in places where the usual lab backbone is weak or absent. If a region lacks stable electricity, highly trained personnel, or specialized machines, a portable test can do more than save time; it can make testing possible in the first place.
Mobile platforms and outbreak response
Beyond individual assays, the review discusses four mobile platforms designed to bring these techniques into real-world outbreak settings. Although the source summary does not list their names in detail, the larger point is clear: diagnostics are increasingly being built as systems, not just standalone tests.
That systems approach matters because successful field testing depends on more than chemistry. Sample handling, power supply, data reporting, biosafety, and transport all affect whether a tool works outside the lab, especially during fast-moving investigations.
Why This Matters
The promise of POCT and PONT is not simply convenience. It is the ability to connect detection directly to action, so clinicians, veterinarians, food inspectors, and public-health officials can make decisions without waiting for a distant lab to weigh in.
That is especially important for surveillance, which the authors frame as one of the main defenses against the spread of infectious disease. Better surveillance starts with better diagnostics, and portable tests can widen the map by bringing reliable detection to places that have historically been hard to monitor.
What comes next
The review presents portable diagnostics as a practical extension of modern outbreak science rather than a replacement for central laboratories. High-capacity labs will still be essential for confirmation, sequencing, and large-scale analysis, but the first signal may increasingly come from a handheld device or a mobile testing setup in the field.
If that transition continues, the biggest change may be cultural as much as technical. Outbreak investigation could shift from a model built around sample transport and delayed answers to one built around local detection, faster feedback, and earlier intervention.