An international study has put numbers on a common but understudied practice in intensive care: giving prokinetic agents, drugs that help move food through the stomach and intestines, to critically ill adults who cannot tolerate feeding well. Researchers followed 1,440 acutely admitted patients in 56 intensive care units across 11 countries and found that 13% received one of these drugs during their ICU stay. The most frequently used medicine was metoclopramide, which accounted for about two-thirds of prokinetic use. Patients who had undergone abdominal surgery before ICU admission were more likely to start these medications, suggesting clinicians may reach for them when the gut is expected to be slow or stressed. The study also found that prokinetic use was associated with a higher rate of serious adverse events, or major harmful events during care, and with fewer days alive outside the ICU and the hospital. At the same time, the drugs were not clearly linked to a difference in 90-day mortality. The authors say the findings offer rare international epidemiology on a treatment that is widely familiar in practice but still supported by limited evidence. Rather than proving the drugs cause harm, the study highlights how often they are used, in whom, and why stronger trials are still needed.
What the study set out to measure
Feeding intolerance is a persistent problem in the ICU. In simple terms, it means a patient's digestive system is not moving nutrition along as expected, much like a traffic jam that keeps supplies from reaching their destination.
For patients receiving tube feeding, that slowdown can matter. If the stomach does not empty properly, it may become harder to deliver enough calories and protein, and clinicians may try drugs that stimulate gut movement to keep feeding on track.
How the PATIENCE cohort was built
The study, called PATIENCE, was designed as an inception cohort study. That means investigators enrolled patients early in a defined clinical course and then observed what happened, rather than assigning treatments the way a randomized trial would.
Between August 2024 and March 2025, the team collected data from acutely admitted adult ICU patients in 56 ICUs spanning 11 countries. They then asked a basic but important question: how many patients actually received a prokinetic agent during their ICU stay?
What the researchers found
Out of 1,440 patients, 187 received a prokinetic drug, for an overall proportion of 13.0%. The median patient age was 64 years, and 56.9% of the cohort was male.
Among the drugs used, metoclopramide was the clear leader, making up 65% of prokinetic treatment. That matters because it suggests one agent dominates practice internationally, even though the broader evidence base for this class remains limited.
Who was more likely to receive these drugs
The clearest baseline factor linked to starting a prokinetic was prior abdominal surgery. The association was measured with a hazard ratio, a statistic that compares how quickly an event happens in one group versus another, and here the hazard ratio was 1.81.
In practical terms, patients with earlier abdominal surgery were substantially more likely to begin prokinetic treatment during their ICU course. That fits bedside logic: if the abdomen has already been operated on, clinicians may expect the gut to be slower to wake up and may intervene earlier.
Safety signals and clinical outcomes
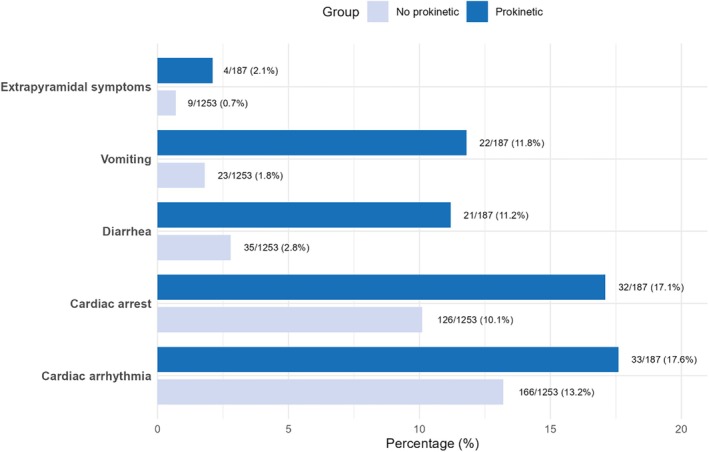
The most attention-grabbing finding was the link between prokinetic use and serious adverse events. Patients who received these drugs had a hazard ratio of 1.9 for experiencing a serious adverse event, meaning the observed rate was nearly twice as high after adjustment for factors such as country, illness severity, comorbidities, surgery, and admission type.
The study also connected prokinetic use to fewer days alive out of the ICU and out of the hospital. The adjusted mean difference was minus 7.6 days alive out of ICU and minus 13.5 days alive out of hospital, suggesting these patients spent longer in high-acuity care or recovered more slowly.
But one major outcome did not show a clear difference: 90-day mortality. The hazard ratio for death by 90 days was 0.62, yet the confidence interval crossed 1.0, meaning the result was not statistically conclusive.
What the numbers do and do not mean
This is where the study needs careful reading. Because PATIENCE was observational, it can show associations but cannot prove that prokinetic drugs themselves caused the worse safety and recovery outcomes.
A simple analogy is an umbrella on a rainy day. Umbrellas are strongly associated with bad weather, but they do not cause the rain; in the same way, prokinetics may be used more often in sicker patients or in patients with harder-to-manage gut problems, even after statistical adjustment.
The authors tried to account for these differences using pre-specified Cox regression and adjusted linear regression models. Those methods help reduce bias, but they cannot remove every hidden difference between treated and untreated patients.
Why This Matters
ICU nutrition is one of those areas where routine practice can get ahead of solid evidence. Clinicians often need to make fast decisions for unstable patients, and prokinetic drugs can seem like a practical tool when feeding stalls.
That is why international data like this are useful. The study shows that prokinetics are not rare edge-case therapies; they were used in roughly one in eight ICU patients in this cohort, and their use clustered in a recognizable subgroup, especially people with prior abdominal surgery.
Just as important, the safety signal means these drugs should not be treated as automatically benign. Even if the association reflects underlying illness rather than direct drug harm, the results make a strong case for closer evaluation of when these agents truly help, which patients are most likely to benefit, and how risks should be monitored.
What comes next
The PATIENCE study offers a clearer map of current ICU practice, but not the final answer on treatment. The next step is likely more targeted research, ideally randomized trials, to test whether prokinetics improve feeding and recovery in specific patient groups without adding avoidable harm.
For now, the message is measured rather than dramatic: prokinetic agents are common, especially after abdominal surgery, and their use tracks with worse short-term clinical outcomes but not a clear difference in 90-day survival. That is enough to justify more scrutiny from critical care teams and more rigorous evidence for a therapy many ICUs already use.